This web page was produced as an assignment for Genetics 564, an undergraduate capstone course at UW-Madison.
What is Spina Bifida?
|
Spina bifida is the most common neural tube defect in the United States. The neural tube is a developmental structure that eventually forms into the spine, spinal cord, and brain. Spina bifida develops during embryonic development when the spinal cord or the protective covering surrounding it (the meninges) fail to form and fuse properly during development. This results in a gap in the spinal cord that can range in severity of appearance and symptoms.[1]
|
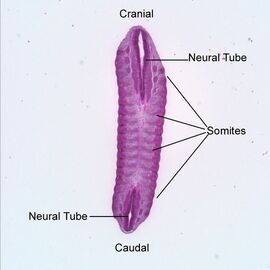
Fig 1. shows the neural tube. The cranial end is toward the head, the caudal end is toward the tail, and somites surround the developing neural tube.
|
Types of Spina Bifida and Associated Symptoms
 Fig 2. Illustration of the types of spina bifida. Spina bifida closed neural tube defects looks similar to occulta.
Fig 2. Illustration of the types of spina bifida. Spina bifida closed neural tube defects looks similar to occulta.
Occulta
Occulta is the most common and mildest form of spina bifida in which a break or malformation is present in the vertebrae. This break is covered by a layer of skin. It is often marked externally by a mole or patch of hair. [1] Spina bifida occulta is generally asymptomatic and is often not detected until late childhood or adulthood. [2]
Closed Neural Tube Defects
Closed neural tube defects is a wide-ranging form of spina bifida. It can include any defect of fat, bone, or meninges that is located on the spinal cord and covered by skin. It is usually asymptomatic but can lead to mobility restrictions, paralysis and/or a dysfunctional bowel and bladder. Externally it looks very similar to occulta but can include a more obvious mark such as an indent in the skin. [1]
Meningocele
Meningocele is a more severe form of spina bifida and is characterized by a protrusion of spinal fluid and meninges through the opening in the vertebrae. This abnormal protrusion may be open or covered by skin. Despite this visible malformation, the underlying nerves generally remain intact, resulting in no neurological symptoms. However, in the case of nerve damage, paralysis and/or dysfunction of the bowel and bladder can occur.[1]
Myelomeningocele
Myelomeningocele is the most severe form of spina bifida. It occurs when the protrusion of meninges and spinal fluid also includes the spinal cord and nerves. This results in partial or complete paralysis of the body below the protrusion due to nerve damage which may prevent walking.[1] Nerve damage can also lead to weakened muscles below the protrusion which can cause developmental malformations such as scoliosis.[3] Nerve damage in the lower spine also can lead to a dysfunctional bowel and bladder. Children with myelomeningocele are also at risk for brain-related complications such as a build-up of fluid around the brain (hydrocephalus), infection of tissues surrounding the brain (meningitis), and brain malformations.[3]
Occulta is the most common and mildest form of spina bifida in which a break or malformation is present in the vertebrae. This break is covered by a layer of skin. It is often marked externally by a mole or patch of hair. [1] Spina bifida occulta is generally asymptomatic and is often not detected until late childhood or adulthood. [2]
Closed Neural Tube Defects
Closed neural tube defects is a wide-ranging form of spina bifida. It can include any defect of fat, bone, or meninges that is located on the spinal cord and covered by skin. It is usually asymptomatic but can lead to mobility restrictions, paralysis and/or a dysfunctional bowel and bladder. Externally it looks very similar to occulta but can include a more obvious mark such as an indent in the skin. [1]
Meningocele
Meningocele is a more severe form of spina bifida and is characterized by a protrusion of spinal fluid and meninges through the opening in the vertebrae. This abnormal protrusion may be open or covered by skin. Despite this visible malformation, the underlying nerves generally remain intact, resulting in no neurological symptoms. However, in the case of nerve damage, paralysis and/or dysfunction of the bowel and bladder can occur.[1]
Myelomeningocele
Myelomeningocele is the most severe form of spina bifida. It occurs when the protrusion of meninges and spinal fluid also includes the spinal cord and nerves. This results in partial or complete paralysis of the body below the protrusion due to nerve damage which may prevent walking.[1] Nerve damage can also lead to weakened muscles below the protrusion which can cause developmental malformations such as scoliosis.[3] Nerve damage in the lower spine also can lead to a dysfunctional bowel and bladder. Children with myelomeningocele are also at risk for brain-related complications such as a build-up of fluid around the brain (hydrocephalus), infection of tissues surrounding the brain (meningitis), and brain malformations.[3]
Causes of Spina Bifida
The onset of spina bifida is a result of many interacting genetic and environmental risk factors. It is not yet known what exact amounts and combinations of risk factors are necessary for spina bifida to develop. Even less is known about the factors that lead to development of a more severe form of the disease or to differing severities of symptoms.
Environmental Risk Factors
Maternal Diet
It is well-established that the presence of folic acid is important for closure of the neural tube during development.[4] Folic acid can be obtained dietarily through eating leafy greens, citrus fruits, beans, and most grains or through a vitamin supplement.[3] However, insufficient folic acid consumption during pregnancy is associated with the development of spina bifida. Some research also suggests that low levels of vitamin B12, which is needed for the body to absorb folic acid, is associated with an increased risk of developing spina bifida. Poor overall nutrition resulting from obesity or poverty has been implicated as an even larger risk factor for spina bifida than folic acid deficiency alone.[4]
Maternal Age and Birth Order
Mothers who are older than 40 or younger than 19 years old are at increased risk of having a baby with spina bifida. Babies who are born into a family that already has children are also more likely to have spina bifida.[5]
Parental Occupational Risks
Parental or maternal exposure to hazardous chemicals such as pesticides is also associated with an increased risk of spina bifida. This risk is highest for repeated exposures which usually is a result of careers such as farming.[5]
Genetic Risk Factors
There are approximately 132 genes that have been identified as possible risk factors for the development of spina bifida. The best studied of these genes is MTHFR.[5]
Environmental Risk Factors
Maternal Diet
It is well-established that the presence of folic acid is important for closure of the neural tube during development.[4] Folic acid can be obtained dietarily through eating leafy greens, citrus fruits, beans, and most grains or through a vitamin supplement.[3] However, insufficient folic acid consumption during pregnancy is associated with the development of spina bifida. Some research also suggests that low levels of vitamin B12, which is needed for the body to absorb folic acid, is associated with an increased risk of developing spina bifida. Poor overall nutrition resulting from obesity or poverty has been implicated as an even larger risk factor for spina bifida than folic acid deficiency alone.[4]
Maternal Age and Birth Order
Mothers who are older than 40 or younger than 19 years old are at increased risk of having a baby with spina bifida. Babies who are born into a family that already has children are also more likely to have spina bifida.[5]
Parental Occupational Risks
Parental or maternal exposure to hazardous chemicals such as pesticides is also associated with an increased risk of spina bifida. This risk is highest for repeated exposures which usually is a result of careers such as farming.[5]
Genetic Risk Factors
There are approximately 132 genes that have been identified as possible risk factors for the development of spina bifida. The best studied of these genes is MTHFR.[5]
The MTHFR Gene
MTHFR is located on chromosome one at position 36.22.[7] It encodes an enzyme called methylenetetrahydrofolate reductase. This enzyme plays a role in several chemical processes within the body by converting the molecule 5,10-methylenetetrahydrofolate into a different molecule called 5-methyltetrahydrofolate.[7] This reaction is an important part of the process of converting dietary folic acid into the amino acid methionine. [6] Methionine is then incorporated into many proteins and has been identified as integral for neural tube closure during development.[7]
Due to the importance of MTHFR for methionine production, a mutation in MTHFR that interferes with healthy gene functioning has been implicated as a risk factor for the development of spina bifida.[8] This mutation is a single nucleotide polymorphism (SNP) that changed the cytosine at position 677 of MTHFR to a thymine.[8] If a baby inherits two copies of this mutation (one from their mother and one from their father), they are two times more likely to develop with spina bifida.[9] This risk can be compounded further by the presence of environmental risk factors mentioned above.[5]
Due to the importance of MTHFR for methionine production, a mutation in MTHFR that interferes with healthy gene functioning has been implicated as a risk factor for the development of spina bifida.[8] This mutation is a single nucleotide polymorphism (SNP) that changed the cytosine at position 677 of MTHFR to a thymine.[8] If a baby inherits two copies of this mutation (one from their mother and one from their father), they are two times more likely to develop with spina bifida.[9] This risk can be compounded further by the presence of environmental risk factors mentioned above.[5]
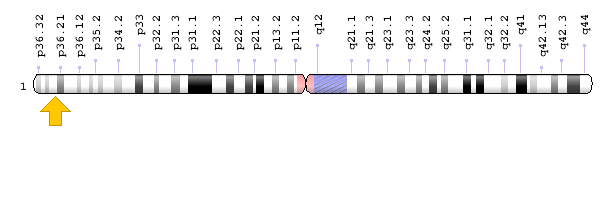
Fig 3. the image above shows chromosome 1. This yellow arrow marks the location of MTHFR on the chromosome.
Detection and Diagnosis of Spina Bifida
 Fig. 4 shows an ultrasound of a baby with myelomeningocele.
Fig. 4 shows an ultrasound of a baby with myelomeningocele.
Spina bifida (other than occulta) is usually detected during prenatal screenings. Spina bifida is one of the birth defects routinely screened for during prenatal check-ups. Although these tests are not 100% reliable, they can give doctors a good indication of a baby's health and if a baby will be affected by spina bifida. Types of prenatal screening include blood tests, ultrasounds, and amniocentesis.[3]
Blood Tests
A blood test called the maternal serum alpha-fetoprotein test is used to check the level of a protein called alpha-fetoprotein (AFP) present in the mother's blood stream. AFP is produced by the baby, and large amounts of it in the maternal bloodstream may indicate the presence of a neural tube defect such as spina bifida. In the case of high AFP levels, a doctor may request an ultrasound.[3]
Ultrasound
An ultrasound is a way for a doctor to view live images of a baby while it is still inside its mother's uterus. Doctors can use these images to look for signs of spina bifida. Indicators they may be able to detect from an ultrasound are breaks in the baby's spine, such as the large bubble present in the ultrasound pictured, as well as malformations of the developing brain.[3]
Amniocentesis
This test is generally only offered if high maternal AFP is detected but the ultrasound does not show clear signs of spina bifida. It is slightly riskier and more invasive than the other tests and involves using a needle to garner a sample of amniotic fluid from the sack that holds the baby. The amniotic fluid will then be tested for AFP. If high levels of AFP are found, it indicates that the baby's neural tube did not fully close and AFP is leaking into the amniotic fluid. This suggests a neural tube defect.[3]
Blood Tests
A blood test called the maternal serum alpha-fetoprotein test is used to check the level of a protein called alpha-fetoprotein (AFP) present in the mother's blood stream. AFP is produced by the baby, and large amounts of it in the maternal bloodstream may indicate the presence of a neural tube defect such as spina bifida. In the case of high AFP levels, a doctor may request an ultrasound.[3]
Ultrasound
An ultrasound is a way for a doctor to view live images of a baby while it is still inside its mother's uterus. Doctors can use these images to look for signs of spina bifida. Indicators they may be able to detect from an ultrasound are breaks in the baby's spine, such as the large bubble present in the ultrasound pictured, as well as malformations of the developing brain.[3]
Amniocentesis
This test is generally only offered if high maternal AFP is detected but the ultrasound does not show clear signs of spina bifida. It is slightly riskier and more invasive than the other tests and involves using a needle to garner a sample of amniotic fluid from the sack that holds the baby. The amniotic fluid will then be tested for AFP. If high levels of AFP are found, it indicates that the baby's neural tube did not fully close and AFP is leaking into the amniotic fluid. This suggests a neural tube defect.[3]
Prevention and Treatment of Spina Bifida
Prevention
The best way to protect against spina bifida and other neural tube defects is to supplement your diet with 400 micrograms of folic acid daily (vitamin B9). It is best to begin dietary supplementation when you begin trying to conceive as supplemental folic acid is vital early in pregnancy to protect against spina bifida. The daily amount recommended is higher for women who are diabetic or taking anti-seizure medication. In these cases a doctor should be consulted.[3]
Treatment
Prenatal Surgery
This is an option when spina bifida is detected through prenatal screening. In this procedure, surgeons repair the baby's spinal cord while they are still in their mother's uterus. This significantly reduces the risk of nerve damage and the associated complications of mobility restriction and bladder/bowel dysfunction. It also can reduce the risk of hydrocephalus. However, this procedure has many risks that should be discussed with a doctor.[3]
Cesarean Birth (C-Section)
Cesarean birth is a surgical delivery of a baby. Delivery by cesarean birth has been associated with lower risk of paralysis in babies with spina bifida. [4]
Surgery After Birth
Babies who are born with meningocele require surgery to replace the meninges back inside the vertebrae and to seal the vertebrae. Generally, there is no damage to the spinal cord which means these babies are at low risk for further complications. Babies who are born with myelomeningocele also need surgery to put the exposed nerves back inside the spine. This reduces the risk of infection and may prevent further nerve damage.[3]
Ongoing Care and Treatment
Babies born with myelomeningocele will likely require ongoing surgeries and care due to the effects of the nerve damage they have sustained. This may include walking aids and physical therapy or a wheelchair for mobility difficulties. It also may include bowel management and surgery for hydrocephalus. There may be additional monitoring and treatment necessary depending on each child's specific needs and complications.[3]
The best way to protect against spina bifida and other neural tube defects is to supplement your diet with 400 micrograms of folic acid daily (vitamin B9). It is best to begin dietary supplementation when you begin trying to conceive as supplemental folic acid is vital early in pregnancy to protect against spina bifida. The daily amount recommended is higher for women who are diabetic or taking anti-seizure medication. In these cases a doctor should be consulted.[3]
Treatment
Prenatal Surgery
This is an option when spina bifida is detected through prenatal screening. In this procedure, surgeons repair the baby's spinal cord while they are still in their mother's uterus. This significantly reduces the risk of nerve damage and the associated complications of mobility restriction and bladder/bowel dysfunction. It also can reduce the risk of hydrocephalus. However, this procedure has many risks that should be discussed with a doctor.[3]
Cesarean Birth (C-Section)
Cesarean birth is a surgical delivery of a baby. Delivery by cesarean birth has been associated with lower risk of paralysis in babies with spina bifida. [4]
Surgery After Birth
Babies who are born with meningocele require surgery to replace the meninges back inside the vertebrae and to seal the vertebrae. Generally, there is no damage to the spinal cord which means these babies are at low risk for further complications. Babies who are born with myelomeningocele also need surgery to put the exposed nerves back inside the spine. This reduces the risk of infection and may prevent further nerve damage.[3]
Ongoing Care and Treatment
Babies born with myelomeningocele will likely require ongoing surgeries and care due to the effects of the nerve damage they have sustained. This may include walking aids and physical therapy or a wheelchair for mobility difficulties. It also may include bowel management and surgery for hydrocephalus. There may be additional monitoring and treatment necessary depending on each child's specific needs and complications.[3]

International Federation for Spina Bifida and Hydrocephalus
Cellebroersstraat 16/Rue des Alexiens 16 B-100 Brussels, Belgium Phone: 0473.326.247 or +32 (0)2 502 0413 https://www.ifglobal.org/ |

Spina Bifida Association
1600 Wilson Blvd, Suite 800 Arlington, VA 22209 Phone: (800) 621-3141 or (202) 944-3285 http://spinabifidaassociation.org/ |
References
[1] Office of Communications and Public Liason: National Institute of Neurological Disorders and Stroke. (n.d.). Spina Bifida Fact Sheet. Retrieved from https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Spina-Bifida-Fact-Sheet#3258_2
[2] Centers for Disease Control and Prevention. (n.d.). What is Spina Bifida?. Retrieved from https://www.cdc.gov/ncbddd/spinabifida/facts.html
[3] Mayo Clinic. (n.d.). Spina Bifida. Retrieved from https://www.mayoclinic.org/diseases-conditions/spina-bifida/symptoms-causes/syc-20377860
[4] Donnan, J., Walsh, S., Sikora, L., Morrissey, A., Collins, K. & MacDonald, D. (2017). A systematic review of the risks factors associated with the onset and natural progression of spina bifida. Neurotoxicology, 61, 20-31. doi: 10.1016/j.neuro.2016.03.008
[5] Au, K.S., Ashley-Koch, A. & Northrup, H. (2011). Epidemiologic and genetic aspects of spina bifida and other neural tube defects. Developmental Disabilities Research Reviews, 16, 6-15. doi: 10.1002/ddrr.93
[6] National Institutes of Health. (n.d.). MTHFR Gene. Retrieved from https://ghr.nlm.nih.gov/gene/MTHFR#location
[7] Essien, F.B & Wannberg S.L. (1993). Methionine but not folic acid or vitamin B-12 alters the frequency of neural tube defects in axd mutant mice. The Journal of Nutrition, 123, 27-34. doi: 10.1093/jn/123.1.27
[8] Wilson, A., Platt, R., Wu, Q., Leclerc, D., Christensen, B., Yang, H., Gravel, R.A. & Rozen, R. (1999). A common variant in methionine synthase reductase combined with low cobalamin (vitamin B12) increases risk for spina bifida. Molecular Genetics and Metabolism, 67, 317-323. doi: 10.1006/mgme.1999.2879
[9] Shaw, G.M., Lu, W., Zhu, H., Yang, W., Briggs, F.B., Carmichael, S.L., Barcellos, L.F., Lammer, E.J. & Finnell, R.H. (2009). 118 SNPs of folate-related genes and risks of spina bifida and conotruncal heart defects. Biomedical Central Medical Genetics, 10, 49. doi: 10.1186/1471-2350-10-49
Images
Header: https://www.medicalnewstoday.com/articles/220424.php
Figure 1: https://officialdress.club/quotes/embryo-day-development-day.html
Figure 2: http://blogs.ubc.ca/earlychildhoodintervention2/2011/02/25/children-with-spina-bifida-sb/
Figure 3: https://ghr.nlm.nih.gov/gene/MTHFR
Figure 4: https://radiopaedia.org/articles/myelomeningocele-1?lang=us
[1] Office of Communications and Public Liason: National Institute of Neurological Disorders and Stroke. (n.d.). Spina Bifida Fact Sheet. Retrieved from https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Spina-Bifida-Fact-Sheet#3258_2
[2] Centers for Disease Control and Prevention. (n.d.). What is Spina Bifida?. Retrieved from https://www.cdc.gov/ncbddd/spinabifida/facts.html
[3] Mayo Clinic. (n.d.). Spina Bifida. Retrieved from https://www.mayoclinic.org/diseases-conditions/spina-bifida/symptoms-causes/syc-20377860
[4] Donnan, J., Walsh, S., Sikora, L., Morrissey, A., Collins, K. & MacDonald, D. (2017). A systematic review of the risks factors associated with the onset and natural progression of spina bifida. Neurotoxicology, 61, 20-31. doi: 10.1016/j.neuro.2016.03.008
[5] Au, K.S., Ashley-Koch, A. & Northrup, H. (2011). Epidemiologic and genetic aspects of spina bifida and other neural tube defects. Developmental Disabilities Research Reviews, 16, 6-15. doi: 10.1002/ddrr.93
[6] National Institutes of Health. (n.d.). MTHFR Gene. Retrieved from https://ghr.nlm.nih.gov/gene/MTHFR#location
[7] Essien, F.B & Wannberg S.L. (1993). Methionine but not folic acid or vitamin B-12 alters the frequency of neural tube defects in axd mutant mice. The Journal of Nutrition, 123, 27-34. doi: 10.1093/jn/123.1.27
[8] Wilson, A., Platt, R., Wu, Q., Leclerc, D., Christensen, B., Yang, H., Gravel, R.A. & Rozen, R. (1999). A common variant in methionine synthase reductase combined with low cobalamin (vitamin B12) increases risk for spina bifida. Molecular Genetics and Metabolism, 67, 317-323. doi: 10.1006/mgme.1999.2879
[9] Shaw, G.M., Lu, W., Zhu, H., Yang, W., Briggs, F.B., Carmichael, S.L., Barcellos, L.F., Lammer, E.J. & Finnell, R.H. (2009). 118 SNPs of folate-related genes and risks of spina bifida and conotruncal heart defects. Biomedical Central Medical Genetics, 10, 49. doi: 10.1186/1471-2350-10-49
Images
Header: https://www.medicalnewstoday.com/articles/220424.php
Figure 1: https://officialdress.club/quotes/embryo-day-development-day.html
Figure 2: http://blogs.ubc.ca/earlychildhoodintervention2/2011/02/25/children-with-spina-bifida-sb/
Figure 3: https://ghr.nlm.nih.gov/gene/MTHFR
Figure 4: https://radiopaedia.org/articles/myelomeningocele-1?lang=us
